Treatment Effects in Stata
Does maternal smoking lower birth weight? Six estimators, one dataset
Nagoya University (GSID)
June 11, 2026
One unadjusted shift — and we cannot yet say what causes it
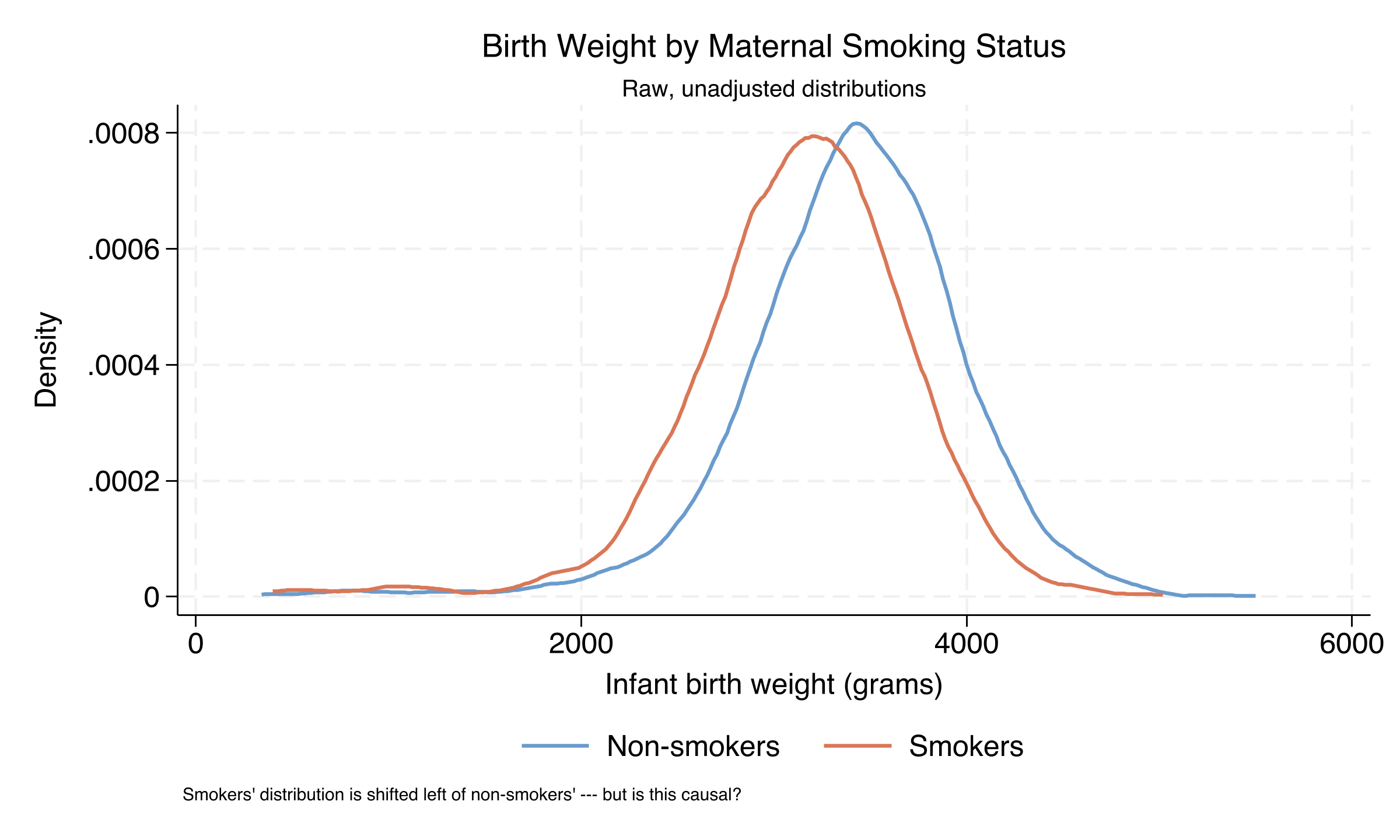
Kernel density of infant birth weight. Smokers’ distribution (orange) sits ~250 g left of non-smokers’ (steel blue) — but the shift conflates smoking with confounders.
Both distributions span (0,1): overlap holds, so IPW is stable
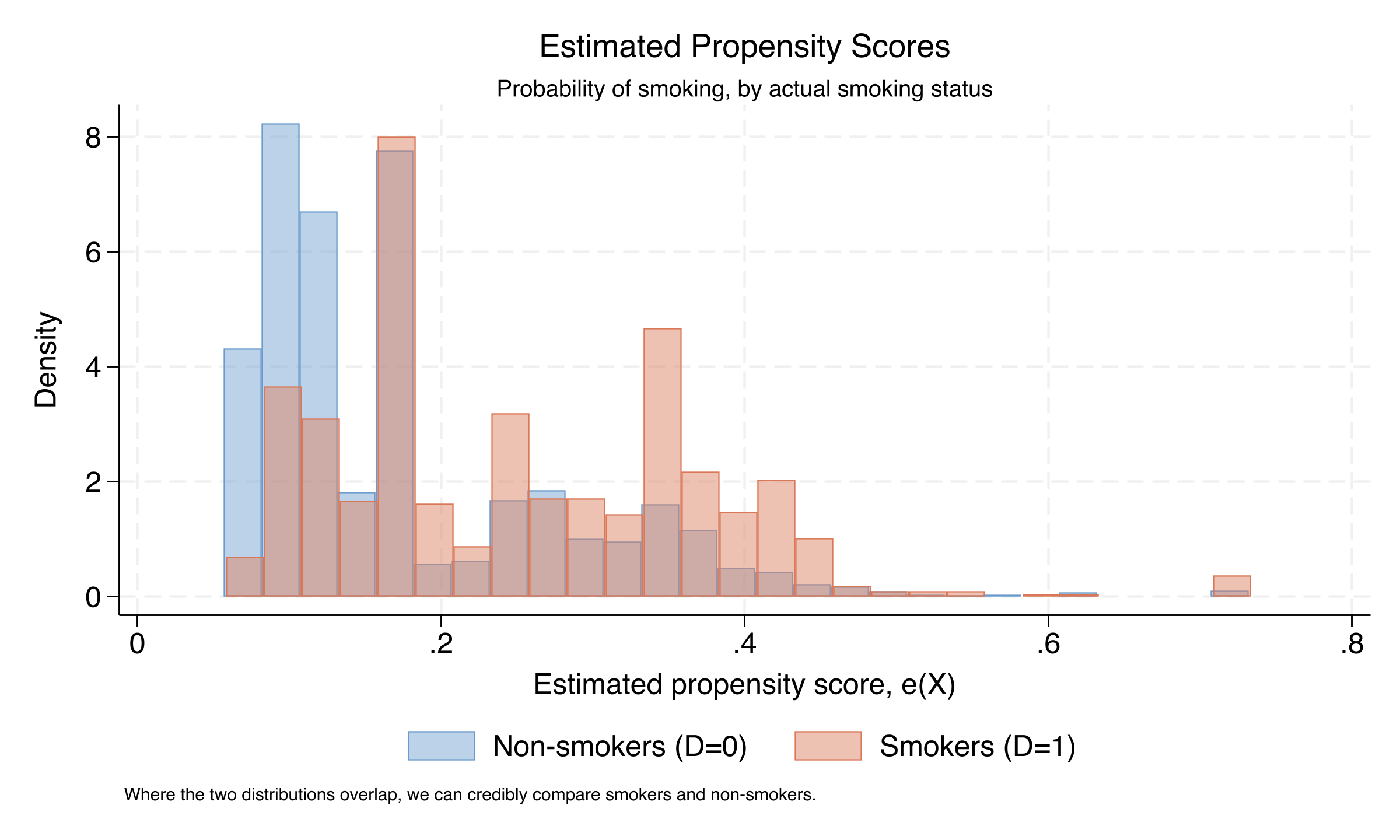
Estimated propensity scores by smoking status. Non-smokers (steel blue) cluster low, smokers (orange) cluster high — but both span most of the unit interval. No zone where one group is absent.
PSM collapses six covariates to one score and matches on it
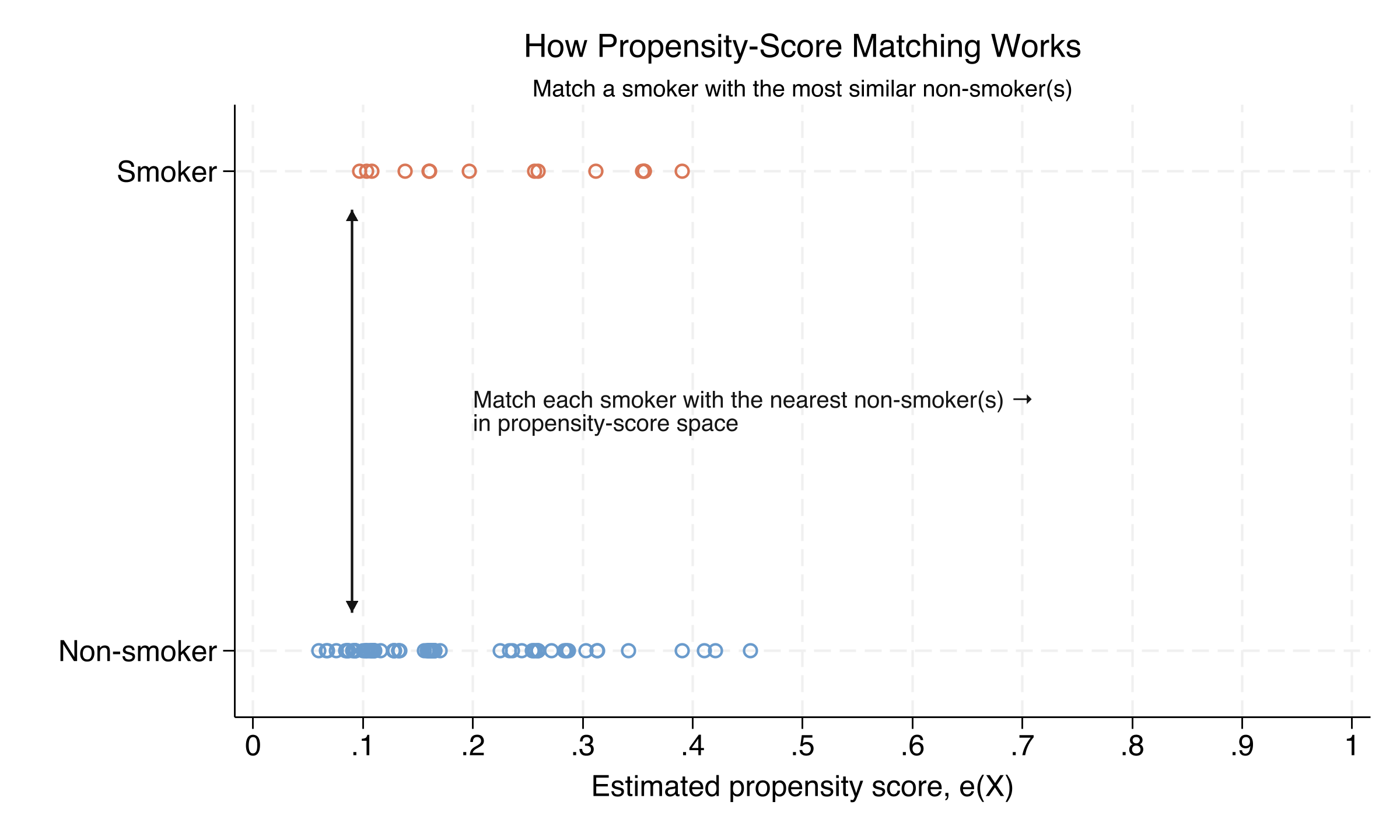
On a 100-mother subsample: each smoker (orange, top row) is matched to the non-smoker(s) with the closest propensity score. Rosenbaum–Rubin: matching on the scalar score balances every covariate that built it.
The forest plot: adjustment rules out the naive −275 g
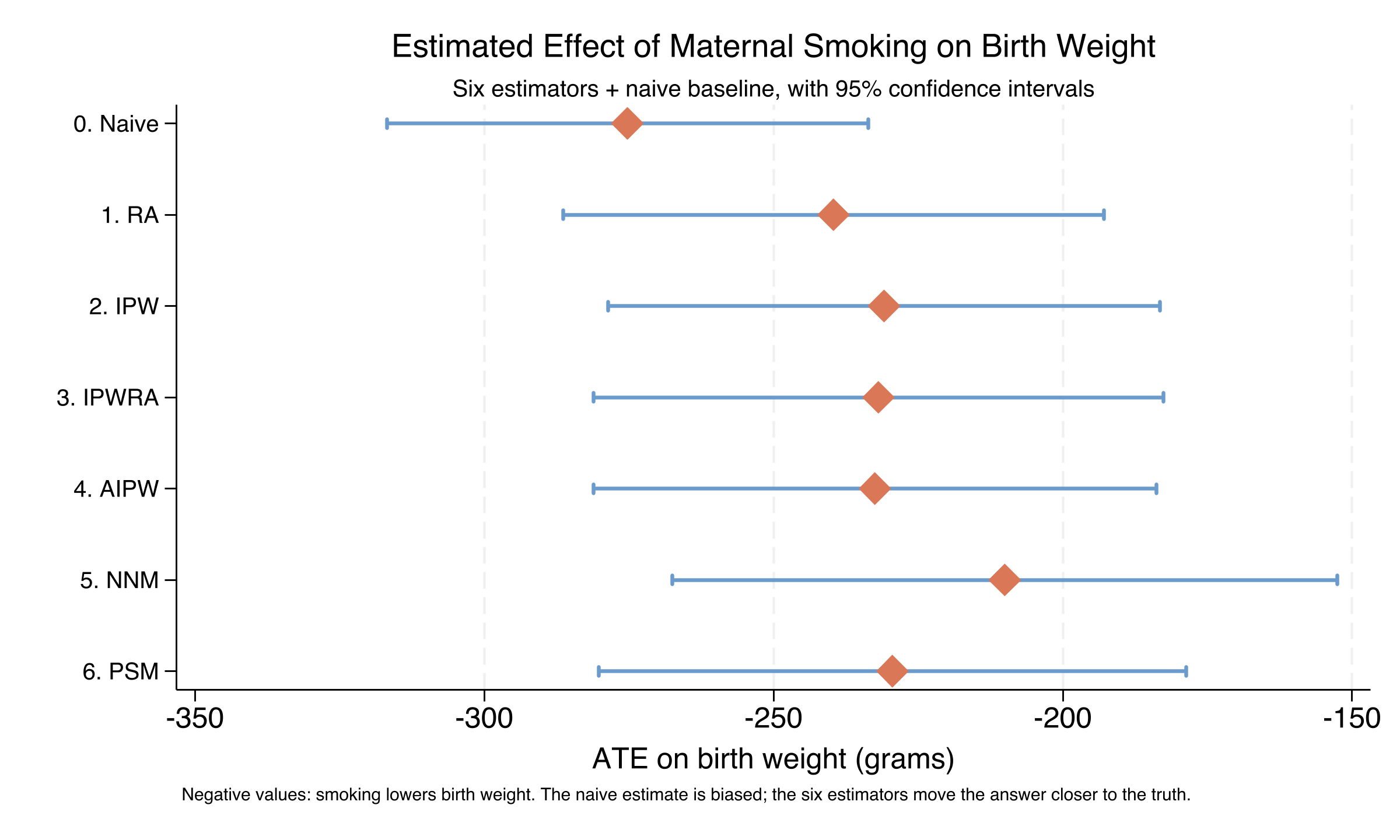
ATE ± 95% CI across seven specifications. The naive estimate (−275 g) is the most negative; six adjusted estimators cluster near −230 g, NNM the slight outlier at −210 g.